Category: Health Sciences and Medicine
ORIGINAL
Investigate the Effect of Using an Adaptable Orthosis with Airbag Cushion as an Arch Support for Flatfoot Treatment
Investigar el Efecto del Uso de una Ortesis Adaptable con Cojín de Airbag como Soporte del Arco para el Tratamiento del Pie Plano
Noor A. Ghassan1 *, Wisam K. Hamdan1 *
1Department of Production Engineering and Metallurgy, University of Technology. Baghdad, Iraq.
2Department of Biomedical Engineering, University of Technology. Baghdad, Iraq.
Cite as: Ghassan NA, Hamdan WK. Investigate the Effect of Using an Adaptable Orthosis with Airbag Cushion as an Arch Support for Flatfoot Treatment. Salud, Ciencia y Tecnología - Serie de Conferencias. 2024; 3:825. https://doi.org/10.56294/sctconf2024825
Submitted: 21-01-2024 Revised: 27-03-2024 Accepted: 02-06-2024 Published: 03-06-2024
Editor:
Dr.
William Castillo-González ![]()
Note: paper presented at the 3rd Annual International Conference on Information & Sciences (AICIS’23).
ABSTRACT
Flatfoot is an abnormality that affects forefoot, midfoot, and hindfoot. This deformity also referred to as pes planus, in which the medial longitudinal arch is collapsed. Flatfoot can be accosted with symptoms such as pain and swelling.
Objective: the aim of this study is to develop an adaptable flatfoot orthosis that uses an airbag cushion to support the arch and help in reducing the pain and improving the pressure distribution.
Methods: the patient went through a physical test and a cast from Plaster bandage was made to the patient’s foot to have the exact foot measurement for the orthosis design. The orthosis was made from two layers, the first layer was made from a Polypropylene sheet as the orthosis base, and the second layer was made from Plastazote. The airbag cushion was placed between the two layers and connected to the air pump. Gait analysis test was carried out on PWALK device with two conditions (with foot orthosis, and without foot orthosis) to test the efficiency of the orthosis.
Results: the gait analysis confirmed that foot orthotics optimize pressure distribution, arch height, and pain reduction during the gait cycle.
Conclusion: our study aims to analyze the benefits of using airbag cushions in flatfoot orthosis. We designed a prototype orthosis with a semi-rigid structure and an airbag cushion to support the arch. The semi-rigid structure allows for normal foot arch mobility, while the airbag cushion helps reduce pain and improve arch height and pressure distribution.
Keywords: Flatfoot; Pes Planus; Adult Acquired Flatfoot; Flatfoot Orthosis; Adaptable Flatfoot Orthosis; Flatfoot Orthosis Design; Airbag Cushion Arch Support.
RESUMEN
El pie plano es una anomalía que afecta al antepié, el mediopié y el retropié. Esta deformidad también se conoce como pie plano, en el que el arco longitudinal medial está colapsado. El pie plano puede cursar con síntomas como dolor e hinchazón.
Objetivo: el objetivo de este estudio es desarrollar una órtesis adaptable para pie plano que utilice un cojín de aire para sostener el arco y ayudar a reducir el dolor y mejorar la distribución de la presión.
Métodos: el paciente se sometió a una prueba física y se le hizo un molde con venda de yeso para obtener la medida exacta del pie para el diseño de la órtesis. La órtesis se fabricó con dos capas, la primera con una lámina de polipropileno como base de la órtesis y la segunda con Plastazote. El colchón de aire se colocó entre las dos capas y se conectó a la bomba de aire. Se realizaron pruebas de análisis de la marcha en el dispositivo PWALK con dos condiciones (con órtesis de pie y sin órtesis de pie) para comprobar la eficacia de la órtesis.
Resultados: el análisis de la marcha confirmó que las órtesis de pie optimizan la distribución de la presión, la altura del arco plantar y la reducción del dolor durante el ciclo de la marcha.
Conclusión: nuestro estudio pretende analizar los beneficios del uso de almohadillas de airbag en ortesis para pie plano. Diseñamos un prototipo de órtesis con una estructura semirrígida y un cojín de airbag para apoyar el arco. La estructura semirrígida permite la movilidad normal del arco del pie, mientras que el cojín de airbag ayuda a reducir el dolor y a mejorar la altura del arco y la distribución de la presión.
Palabras clave: Pie Plano; Pes Planus; Pie Plano Adquirido en el Adulto; Ortesis para Pie Plano; Ortesis Adaptable para Pie Plano; Diseño de Ortesis para Pie Plano; Cojín Airbag de Soporte del Arco.
INTRODUCTION
Flatfoot, also known as pes planus, is a term used to describe foot deformity that can be symptomatic or not. People with flatfoot will have a fallen medial longitudinal arch, affecting the forefoot, midfoot, and hindfoot.(1) The tendon of the peroneus longus, which runs from lateral to medial across the pedis and attaches to the proximal end of the first metatarsal bone, works in conjunction with the tendons of the tibialis anterior and posterior muscles to hold the load of the arches very effectively.(2) Flatfoot may be developmental in nature, expressed in childhood, or acquired, expressed in adulthood. Based on the condition flatfoot can be either rigid or flexible. Rigid flatfoot condition means that there is no arch in case of standing or sitting, while flexible flatfoot means that there is no arch only in case of standing. However, flatfeet can affect one foot or both feet. On the other hand, flatfoot can have symptomatic or asymptomatic.(1) Acquired adult flatfoot is an abnormality caused by repetitive overloading which affects the foot arch, leading to progressive tibialis tendon (PTT) insufficiency.(3) It is considered a common foot deformity that is developed during adulthood (after skeletal maturity). Acquired flatfoot may be partial or complete flattening of the arch.(4) Flatfoot can be treated by either surgical procedure or non-surgical procedure that include using flatfoot orthosis (FOs). A number of studies investigated how effectively flatfoot orthoses manage the symptoms of flatfoot, and it was found that flatfoot orthosis was optimizing plantar pressure, improving body stability and enhancing sports biomechanical performance in children and adults with flexible flatfoot.(5) Another researcher found that the foot orthosis also decreased the maximum ankle eversion angle and ankle eversion moment and improving foot alignment during walking.(6) The design and materials of flatfoot orthoses have also been a topic of debate. It was discovered that the materials polyurethane (including PORON®), polyethylene (including Plastazote®), ethyl vinyl acetate (EVA), and polyurethane (including PORON®) could lower peak pressure in different areas of the foot.(7) In terms of orthosis structure, it was found that rigid foot orthoses limited the foot mobility, while the simi-rigid structure facilitate the foot mobility.(8) There are different types of foot orthotics such as, 3D-printed FOs, which are successful in preventing arch height decrease,(9) and it could be a good substitute for traditional plaster-molded (TPM) foot orthoses in clinical settings.(10) CAD-CAM and prefabricated foot orthosis that improve the planter pressure distribution.(11) Foot taping which can be used to predict the biomechanical results of a foot orthoses intervention depending on the reaction to foot tape.(12)
METHOD
In this section, we will explain the process of designing and developing the orthosis. We developed a flatfoot orthosis that support the arch by an airbag cushion, that can reduce the pain and improve the pressure distribution.
Flatfoot Orthotic Designs Steps
Assessment of the patient’s foot and gait: the patient went through a physical test at Al-Ibtisam Center for Prosthetic Limbs and Supports in order to diagnoses the deformity level, type of flatfoot, and arch height. The applied test involves walking with and without the shoes, rise on heels test, checking the body alignment and taking foot measurements (length, width, desired arch height, and weight) as shown in figure 1, the patient measurements are shown in table 1. The patient (female, age 28) was diagnosed with flexible adult acquired flatfoot; stage IIa with hindfoot valgus in the right foot. Flatfoot was causing pain in the back and neck of the patient and can lead cervical or dorsal spondyloptosis in future.
|
Table 1. Patient Measurements |
|
|
Patient Measurements |
|
|
Length |
24 [cm] |
|
Width |
10 [cm] |
|
Weight |
54 [Kg] |
|
Desired arch height |
2,5 [cm] |

Figure 1. Physical test and foot measurement
Casting or scanning the foot: after the examination is over, we use the traditional method for creating a mold from Plaster bandage that shown in the figure 2.

Figure 2. Plaster bandage
The first step was to immerse the Plaster bandage in the water for 2 sec. As illustrated in figure 3 a piece of metal was placed over the leg, so we can cut the mold without hurting the leg. Foot and leg were covered with Nylon as the first layer and followed with four layers of the Plaster bandage.

Figure 3. Covering process with Plaster bandage
We made a longitudinal incision in the cast using a cutter; the incision was made over the metal piece to ensure that no harm will be caused to the leg, as shown in figure 4.

Figure 4. Cutting the cast
The cast was filled with Borax; the Borax was firstly mixed with 3 liters of water. After filling the cast, it was left for half hour to solidify. As illustrated in figure 5 the cast was grinded using smoothing file tools that shown in the figure 6.

Figure 5. Smoothing the cast

Figure 6. Smoothing file tools
Choosing the appropriate materials: for the orthotic base we select Polypropylene that shown in the figure 7. Depending on the previous studies, orthosis that use Polypropylene provide good results with less stress and deformation, also it have a good safety factor,(13,14) low cost,(15) also it has a significant favorable effect on the joint kinetics of gait during level ground walking(13,14) and improve the pressure distribution.(16) The base was covered by Plastazote sheet that shown in the figure 8 since this thermoplastic polyethene foam moulds itself to the contours of the foot when walking to give a relief and cushions pressure areas of the foot,(7) also it helps in reducing the pressure distribution, sheer force and braking force.(17)

Figure 7. Polypropylene sheets
Figure 8. Plastazote sheets
Designing the shape of the orthotics: for our patient case, since the right foot suffer from hindfoot valgus, we planned to design a half-length orthotics for the right foot only. The first step was annealing process to the Polypropylene sheet at 255 °C for 15 minutes using cabinent oven C.5000 that shown in the figure 9.

Figure 9. Annealing process for the Polypropylene sheet
Secondly, we cover the cast with Nylon to form a protective layer from humidity, dust, heat, and to remove the annealed sheet from the cast after the forming process. The second layer was from Perlon stockinette to form a thermal insulator and to provide a smooth finishing. The orthotics base was made by drawing the annealed Polypropylene sheets over the cast and removing the excess materials. Finally, we added the airbag cushion on its predefined position to support the arch as in figure 10.

Figure 10. Designing the orthosis base
The last step, was to cover the orthosis with the Plastazote sheet, adding the fixture strips that made from velcro tape, it was attached to the orthotics using snap buttons, We used a drilling machine to create the holes for the snap buttons. We connect the airbag cushion with the air pump (we used mercurial sphygmomanometer pump). Figure 11 shows the designed orthotics.

Figure 11. Flatfoot orthosis with airbag cushion as an arch support
Orthosis Fit and Evaluation: the orthosis must be modified once it has been made to achieve a correct fit. To ensure that the orthosis offers the optimum degree of support and comfort. Although the orthosis achieved a correct fit to the patient’s foot, the patient will need to wear a sports shoe that is larger from her original foot size with 2-3 degree. The patient wares the orthosis for 5 months on daily basis.
Gait Analysis Test: gait analysis test was preformed using PWALK device at Alshaea clinic, that is shown in the figure 12 to determine the effect of the orthosis on the pressure distribution; the test was applied with two condition (walking without the foot orthosis, and with the foot orthosis) as shown in figure 13.

Figure 12. PWALK device

Figure 13. Gait analysis test, (a) gait analysis test without foot orthosis, (b) gait analysis test with foot orthosis
RESULTS
Gait analysis test was preformed using PWALK device to determine the effect of the orthosis on the pressure distribution; the test was applied with two condition (walking without the foot orthosis, and with the foot orthosis). In figure 14, we can notice that the left foot was classified as high arch foot, while the right foot was classified as heavy high arch foot (with foot orthosis), as in figure 15.

Figure 14. Results of the giat anaylsis that define the left foot as high arch foot

Figure 15. Results of the giat anaylsis that define the right foot as heavy high arch foot
For the pressure distribution, in case 1 (without the foot orthosis) the patient apply more pressure on her left foot, the average pressure on the left foot was (135,3 Kpa) and (119,3 Kpa) for the right foot, as illustrated in figure 16.

Figure 16. Pressure distrbution without foot orthosis
The results that shown in figure 17 which represent case 2 (with the foot orthosis), also shows that the patient applied more pressure on the left foot, the average pressure on the left foot was (106 Kpa) and (74 Kpa) for the right foot. Compared to the results of case 1, we can notice that the pressure on both feet was reduced, which approve that the orthosis improved the pressure distribution. Furthermore, the pressure distribution can be better when using airbag cushion for both feet even if one of the feet was normal foot. According to the pressure distribution during the gait cycle and duration variation of each cycle the patient suffered from hindfoot valgus in the right foot, that mean there was no significant change in the hindfoot valgus.
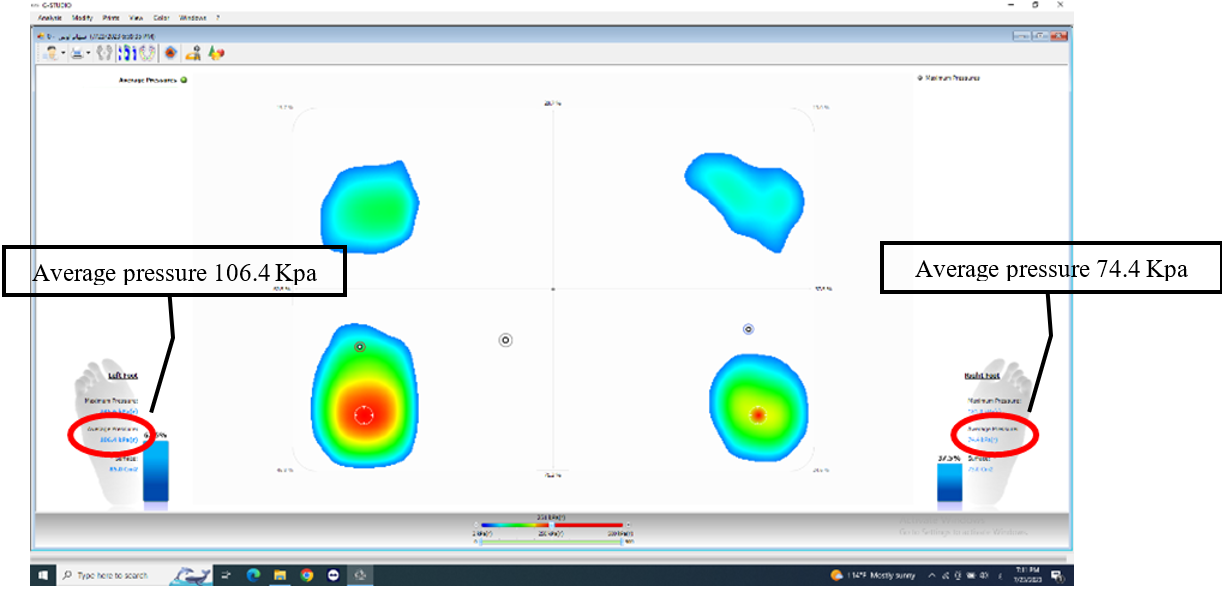
Figure 17. Pressure distrbution with the foot orthosis
CONCLUSIONS
In this study, we investigate the effect of using airbag cushion in flatfoot orthosis. A prototype orthosis was designed with simi-rigid structure and an airbag cushion as an arch support for the right foot only since the left foot was normal foot. The simi-rigid structure facilitate foot mobility in the normal range of the foot arch, while the airbag cushion helps in reducing pain and improving the arch height, so the foot was considered as heavy high foot arch. The pressure distribution was seems to be better when using the foot orthosis and we can obtain better results when using the orthosis for both feet. On the other hand, the gait analysis results shows that there was no significant change in the hindfoot valgus, which mean that the orthosis was able to control the misalignment to not increase. There was some limitation in the design including the general appearance that make it hard to be used in daily life.
REFERENCES
1. P. McCormack, R. P. Ching, and B. J. Sangeorzan, “Biomechanics of procedures used in adult flatfoot deformity,” Foot Ankle Clin, vol. 6, no. 1, pp. 15–23, Mar. 2001, doi: 10.1016/S1083-7515(03)00072-X.
2. T. Kobezda, “The role of the foot in the mechanism of shock absorption,” Biomechanica Hungarica, May 2009, doi: 10.17489/biohun/2009/1/04.
3. Polichetti et al., “Adult Acquired Flatfoot Deformity: A Narrative Review about Imaging Findings,” Diagnostics, vol. 13, no. 2, p. 225, Jan. 2023, doi: 10.3390/diagnostics13020225.
4. V. Flores, C. Mejía Gómez, M. Fernández Hernando, M. A. Davis, and M. N. Pathria, “Adult Acquired Flatfoot Deformity: Anatomy, Biomechanics, Staging, and Imaging Findings,” RadioGraphics, vol. 39, no. 5, pp. 1437–1460, Sep. 2019, doi: 10.1148/rg.2019190046.
5. Wegener, A. E. Hunt, B. Vanwanseele, J. Burns, and R. M. Smith, “Effect of children’s shoes on gait: a systematic review and meta-analysis,” J Foot Ankle Res, vol. 4, no. 1, p. 3, Dec. 2011, doi: 10.1186/1757-1146-4-3.
6. Y. Peng et al., “Immediate Effects of Medially Posted Insoles on Lower Limb Joint Contact Forces in Adult Acquired Flatfoot: A Pilot Study,” Int J Environ Res Public Health, vol. 17, no. 7, p. 2226, Mar. 2020, doi: 10.3390/ijerph17072226.
7. J. M. Gerrard, D. R. Bonanno, G. A. Whittaker, and K. B. Landorf, “Effect of different orthotic materials on plantar pressures: a systematic review,” J Foot Ankle Res, vol. 13, no. 1, p. 35, Dec. 2020, doi: 10.1186/s13047-020-00401-3.
8. R. Sheykhi-Dolagh et al., “The influence of foot orthoses on foot mobility magnitude and arch height index in adults with flexible flat feet,” Prosthet Orthot Int, vol. 39, no. 3, pp. 190–196, Jun. 2015, doi: 10.1177/0309364614521652.
9. M. Ho, J. Nguyen, L. Heales, R. Stanton, P. W. Kong, and C. Kean, “The biomechanical effects of 3D printed and traditionally made foot orthoses in individuals with unilateral plantar fasciopathy and flat feet,” Gait Posture, vol. 96, pp. 257–264, Jul. 2022, doi: 10.1016/j.gaitpost.2022.06.006.
10. S. Mo et al., “The biomechanical difference between running with traditional and 3D printed orthoses,” J Sports Sci, vol. 37, no. 19, pp. 2191–2197, Oct. 2019, doi: 10.1080/02640414.2019.1626069.
11. B. Khodaei, H. Saeedi, M. jalali, M. Farzadi, and E. Norouzi, “Comparison of plantar pressure distribution in CAD–CAM and prefabricated foot orthoses in patients with flexible flatfeet,” The Foot, vol. 33, pp. 76–80, Dec. 2017, doi: 10.1016/j.foot.2017.07.002.
12. C. BISHOP, J. B. ARNOLD, and T. MAY, “Effects of Taping and Orthoses on Foot Biomechanics in Adults with Flat-Arched Feet,” Med Sci Sports Exerc, vol. 48, no. 4, pp. 689–696, Apr. 2016, doi: 10.1249/MSS.0000000000000807.
13. S. Jena, T. Arunachalam, and S. K. Panda, “Experimental and numerical investigation of a polypropylene orthotic device for assistance in level ground walking,” Proc Inst Mech Eng H, vol. 234, no. 4, pp. 356–369, Apr. 2020, doi: 10.1177/0954411919894091.
14. G. Y. GAUTAM, M L JAIN, and VIJAY GEHLOT, “DESIGN AND ANALYSIS OF THERMOPLASTIC POLYPROPYLENE ANKLE FOOT ORTHOSIS,” Journal of Manufacturing Engineering, vol. 16, no. 3, pp. 087–091, Oct. 2021, doi: 10.37255/jme.v16i3pp087-091.
15. S. Raghvan, P. Singhal, R. K. Diwan, and S. Rattan, “Polypropylene/glass fiber/ethylene propylene diene ternary composites with improved thermoforming properties for orthotic aids,” 2021, p. 020045. doi: 10.1063/5.0063648.
16. S. Jena, T. Arunachalam, and S. K. Panda, “Experimental and numerical investigation of a polypropylene orthotic device for assistance in level ground walking,” Proc Inst Mech Eng H, vol. 234, no. 4, pp. 356–369, Apr. 2020, doi: 10.1177/0954411919894091.
17. Kermen and H. Mohammadi, “Mechanics of foot orthotics: material properties,” J Med Eng Technol, vol. 45, no. 8, pp. 627–641, Nov. 2021, doi: 10.1080/03091902.2021.1940332.
FINANCING
The authors did not receive financing for the development of this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Noor A. Ghassan, Wisam K. Hamdan.
Data curation: Noor A. Ghassan, Wisam K. Hamdan.
Formal analysis: Noor A. Ghassan, Wisam K. Hamdan.
Research: Noor A. Ghassan, Wisam K. Hamdan.
Methodology: Noor A. Ghassan, Wisam K. Hamdan.
Drafting - original draft: Noor A. Ghassan, Wisam K. Hamdan.
Writing - proofreading and editing: Noor A. Ghassan, Wisam K. Hamdan.